 |

08 Apr 2009
Light as a therapy can heal injuries and reduce pain in humans and animals. James Carroll of THOR Photomedicine discusses the rapidly growing field of low level laser therapy.
In science fiction films, when someone gets injured they are taken to a hospital where the doctor uses a laser beam to heal the patient. This might seem unbelievable at first but the use of laser and LED light for tissue regeneration is already advanced in development and used by hundreds of pioneering doctors around the world. The use of laser and LED light as a therapy is called low level laser therapy (LLLT). These therapy systems are already being used to treat wounds, injuries, neck pain, osteoarthritis, the side effects of chemotherapy and radiotherapy, to name but a few.

LLLT is being trialled on NASA manned missions into space and has been used in Antarctica and on US Navy submarines as, in these extreme environments, people do not heal very well after injury. Scientists are currently investigating the use of LLLT on sperm mobility, spinal cord injuries, stroke, and both Parkinson's and Alzheimer's disease. It is anticipated that this technology could be used in almost every hospital department throughout the world, bringing science fiction into reality.
Photosynthesis for humans
It is a common misconception that all medical laser treatments are destructive or tissue-heating procedures (such as cauterizing, ablating or excising tissue). The effects of LLLT are not thermal, they are photochemical. It is not a destructive procedure, it is comparable to photosynthesis.
One of the primary effects of LLLT occurs in the "power house" of human cells – the mitochondria. Certain wavelengths of light stimulate the enzyme cytochrome c oxidase, which is responsible for the production of the essential cellular energy (ATP) that human cells need to function, as well as modulating other biochemical molecules (reactive oxygen species and nitric oxide) that lead to ageing and cell death (oxidative stress). After LLLT, the cells have increased metabolism, they communicate better and they survive stressful conditions better, which in turn suggests that any disease or injury could potentially be influenced.
Dozens of universities across the world are publishing research and demonstrating improved tissue regeneration (in skin, muscle, tendon, ligament, bone, spinal cord and nerve tissue), anti-inflammatory effects and analgesia. A search on the US National Institute of Health online database (www.pubmed.gov) finds over more than 100 randomized double-blind placebo-controlled clinical trials and more than 1000 laboratory studies reporting on the phenomena of LLLT.
At BiOS 2009 (part of SPIE Photonics West) invited speakers from NASA, the US Navy, Harvard Medical School, the former editor of Grays Anatomy and I were among a dozen others who delivered our latest results and thoughts on the effect of LLLT on intracellular mechanisms and its clinical benefits. Research was presented on the effects of this modality for stroke recovery, restoring eyesight after laser injury, healing age-related macular degeneration, improving heart muscle after myocardial infarction, spinal cord injuries, sperm motility and my topic of dose rate effects.
The significance for patients and healthcare services is potentially huge. LLLT is proving to be more effective and cheaper than current drug therapies for many chronic, degenerative or painful conditions. It often works where drug therapies do not and has no side effects.
Laser patch technology
The laser and LED sources used for LLLT are typically between 600 and 950 nm. Irradiance is in the range from 5 mW/cm2 to 1 W/cm2. Irradiation times range from 10 s to 10 min. Treatment intervals may be as often as daily or as infrequent as monthly until the injury has healed. Occasionally just a single treatment is necessary.
There is an opportunity for a manufacturer to bring a disposable, stick-on patch-type laser or LED array to market for the home. Such a prescribeable device could be programmed to deliver appropriate bursts of light at specific wavelengths for certain durations at certain intervals to treat superficial injuries and joint pains.

Controversies and challenges
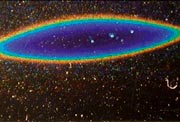
A confounding factor in LLLT research is laser beam measurement. Biologists performing in vitro (petri dish) studies are mostly unaware that the cells in the centre of the dish are receiving a higher irradiance than those on the outside because of the inhomogeneous beam profile. Diode laser beams are not round (they are roughly elliptical) and the power distribution is uneven, depending on whether a single or multimode diode laser is used.
A lack of discussion and understanding among LLLT research academics (biologists and physicians) has meant that no methods have been agreed or standards set for defining the area of a beam. Some report the diameter of the aperture of the apparatus while some have measured the beam dimensions with a ruler. This leads to vastly inconsistent reporting and therefore variable results. This problem could be resolved by adding lenses, light pipes and diffusers to create a more homogeneous flat-top distribution of light across the dish.
Output performance changes as a diode laser heats up. Most laser systems used in laboratory research are clinical LLLT units with no heat or output management. These systems are designed to be used for just a few minutes in clinics but laboratory experiments can take over an hour of continuous use. This means that the output delivered may have diminished by the end of an experiment, leading to different cellular responses and misleading conclusions.
LLLT versus pharmaceuticals
Unlike pharmaceutical research, LLLT has been almost entirely a university endeavour where every success and every failure has been published. Compared with well funded drug therapies where failures are kept behind corporate doors, LLLT failures are often published as university departments are under pressure to publish. This does not mean that LLLT does not work; it just means that the parameters were wrong and, as we know, there are many to choose from. More research has been conducted with LLLT on osteoarthritis than with non-steroidal anti-inflammatory
drugs (the standard prescribed drug). LLLT is cheaper, safer and frequently more effective than drug therapies and yet your doctor has probably never heard of it.
Most people who are suffering from pain, soft tissue injury, osteoarthritis or a chronic illness would prefer to take fewer pharmaceuticals – especially considering the potential side-effects of many medications. However, until government funding prioritizes research and development into these types of safer, effective, non-costly, non-invasive modalities in the UK, we will continue to give patients less than optimal treatment. The UK has many scientific experts but they all work overseas as the funding and support is available there rather than here. We must support our scientists and medical community in furthering UK research and development in crucial areas like this.
According to Dr Kevin Moore, an anaesthetist at the Royal Oldham Hospital and a specialist in chronic pain, "Any pain clinic that does not have access to LLLT is offering less than optimal treatment."
LLLT is the medicine of the future. What's missing now is the right mix of vision, home-use technology and funding to make this a billion pound industry.
• This article originally appeared in the April 2009 issue of Optics & Laser Europe magazine.
View PDF of article
 |  |  |  |  |  |  |
| © 2026 SPIE Europe |
|




